Let’s make a general but factual statement. Ketosis is not dangerous. Ketoacidosis is dangerous. Many people often confuse the two conditions. They are not the same thing!
Ketosis
Ketosis is a metabolic state in which your body uses ketone bodies in the blood as fuel, derived from fatty acids, in contrast to a glycolysis state where it uses blood glucose (otherwise known as sugar) for energy. The level of ketones during ketosis are typically low in contrast to much higher levels in Ketoacidosis. Ketosis is a normal process in the body. Ketosis may be safely achieved by eating a diet very low in carbohydrates, otherwise known as a ketogenic diet.
Ketoacidosis (DKA)
Ketoacidosis or diabetic ketoacidosis (DKA) is a life-threatening condition that results as a complication of Type 1 Diabetes and may occur in unmanaged Type 2 Diabetes. It occurs when there are dangerously high levels of ketones and blood sugar present at the same time. The take away here is the “and”. It is important to understand that DKA depends upon a very high state of hyperglycemia, typically higher than 250mg/dl and very high levels of ketones. For reference, normal fasting blood glucose (FPG) is 80-100mg/dl. Such high levels of ketones are not typically achievable if adhering to a ketogenic diet and keto diets are low sugar diets so DKA is highly unlikely.
The combination of having too many ketones and too much glucose present in your blood makes it become highly acidic. This can result in damage to the normal functioning of your kidney and liver. Anyone suspected of experiencing DKA should medical treatment immediately.
Ketoacidosis can be triggered by improper diet, infection or illness which may elevate blood glucose, and improper doses of insulin in diabetic patients. Most patients, in my experience treating hundreds of people with DKA, develop DKA due to a diet high in carbs & sugar and without proper insulin management and also when alcohol intoxicated.
What are Ketones?
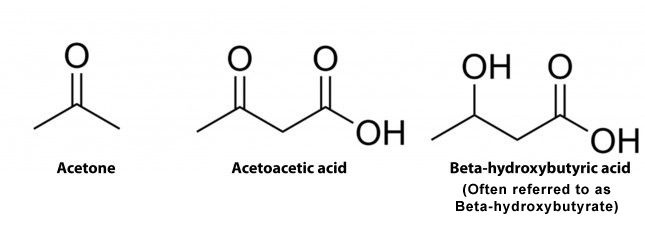
Ketones are compounds that are produced when the body uses fat instead of sugar as fuel. It is more properly described as three molecules, AcetoAcetate, BHB, and acetone. During a proper ketogenic diet, very little carbs and/or sugar is consumed. Without the dietary consumption of carbs/sugars, the body will have little choice but to utilize fatty acids as an alternative fuel source. Ketones are made as a byproduct of processing fatty acids in the liver. Almost all of us have an untapped resource of fat in our bodies to tap into for energy.
Are Ketones Normal?
Yes, we all have and use ketone bodies, in various levels, when in a fasted state like when we wake up in the morning and during/after prolonged and/or intense exercise. Ketone bodies are used as a very efficient and almost unending fuel source by our bodies and our brains when utilizing a ketogenic diet low in carbs.
So why the confusion?
First of all, Ketosis and Ketoacidosis sound a lot alike don’t they? Unless you’re a medical geek, advanced Nurse or Doctor, you probably don’t know they are very different. The difference is two-fold. In ketosis, blood sugar remains normal to low normal. In DKA, blood sugar is very high. More importantly, in ketosis, blood pH remains normal. During DKA, the blood pH is acidic, hence the give-away suffix “Keto-acidosis”. During a normal physiologic pH, our kidneys filter and reabsorb ketone bodies. These normal levels of ketone bodies dissociate completely, and the kidneys do not become overwhelmed.
In a state of DKA, the physiologic pH becomes acidic and rapidly overwhelms the kidneys normal buffering capacity and leads to a condition called metabolic acidosis. Other harmful things will occur like hyperkalemia and increased anion gap, but that is beyond the scope of this post.
Again, a ketogenic diet will not produce a sufficient amount of ketones to achieve DKA and without the consumption of carbs/sugars, the body will not have the opportunity to have a dangerously elevated FPG.
How does this work with Diabetics?
Type 1 Diabetics (T1D) do not produce or produce very little insulin by their pancreas. They are insulin-dependent patients, that is, they must regulate their FPG by exogenous injection of a combination of long acting and short acting insulin.
Type II Diabetics (T2D) do produce insulin. T2D’s become Diabetic not because of an insulin dysfunction per se, but because their bodies produce too much insulin (hyperinsulinemia) over a long period of time. The state of hyperinsulinemia is in response to chronically elevated blood glucose levels from over-consumption of carbs and sugars. T2D is the pre-cursor to a host of other conditions like high blood pressure, heart disease, neuropathy, and cognitive disorders along with, of course, Obesity, Fatty Liver disease and Hypertriglyceridemia. Otherwise known as metabolic syndrome.
T1D’s may benefit greatly from a ketogenic diet. Recall that in T1D’s who encroach upon DKA, both glucose and ketones are high, primarily due to a pathologic lack of insulin. In this situation, ketones are not burned for fuel but rather pile up like a heap of garbage. In a ketogenic diet, ketone requirements go up and glucose requirements go down. The body utilizes ketones for fuel instead of glucose. There is less of a need for injecting exogenous insulin so therefore insulin requirements go down. This is all due to a diet low in carbs/sugar.
Whether you are T1D or T2D, if the body has no choice, given very little glucose resource while eating a ketogenic diet low in carbs/sugar, it will resort to burning fat by breaking down fatty acids and using the byproduct of ketone bodies for fuel. By following a ketogenic diet, many T2D’s can effectively stop and reverse their T2D simply by changing their dietary lifestyle. Similarly, T1D’s will also benefit from having decreased insulin requirements beyond their morning maintenance bolus. Decreasing a T1D’s insulin requirements, based on dietary carb reduction, will result in fewer long-term complications associated with T1D, as mentioned above. T1D’s can’t change the fact that their Pancreas doesn’t produce insulin, but they can drastically improve their quality of life by reducing their consumed carbs/sugars with a ketogenic diet.
I’ll die without my carbs?
No, you will not die. Our bodies are remarkably equipped to produce all the glucose needed to function properly without relying on the consumption of glucose. Our bodies have evolved ways of survival simply by reversing the process of glycolysis (burning carbs/sugar) to make new glucose from fatty acid oxidation (gluconeogenesis) in the liver. No consumed glucose is needed. This is one reason ketogenic diets are used with pediatric patients who suffer from chronic uncontrolled seizures. They need not rely on consuming a diet which contains high amounts of carbs/sugar because their bodies produce glucose in sufficient amounts as needed to supply the brain and the CNS.
But my Doctor says…
Yes, I know. You’re Doctor told you that keto diets may cause ketoacidosis. My advice to you is don’t argue but find a second opinion. Doctors are humans too and many simply don’t understand the process quite fully yet. After all, medicine is a practice, not an exact science so don’t feel guilty to question your white coat advisor. He/she may learn a thing or two from you if you take the opportunity to educate yourself about your disease and find ways to help control or reverse it. The medical community was just as duped as we were by the false diet-heart cholesterol model. Many still are.
Is it dangerous?
I always say, eating too any green beans can be dangerous if you eat nothing but green beans by the pound. My recommendation is for you to put your researcher hat on. Sit down and start your search. These days there are vast fields of virtual information about ketogenic diets out there. Talk to someone who’s doing it. Try to better understand your disease and then sit down with your Doctor. Have a serious conversation with them. Tell them you really want to own it and do what is necessary to get better. If their answer doesn’t sit well with you then find another Doctor.
As always, when starting a lifestyle change, make sure you are being managed by a Doctor or someone trained to help you. If you are T1D, you will need to really hone in your monitoring skills and make sure your insulin intake is being managed appropriately. As your daily glucose levels drop, so will your need to counteract that glucose with insulin. Too much insulin will drop your blood sugar to very low levels and you will get yourself into a medical emergency. Don’t do that!
If you are still concerned about ketone levels then take the guess work out of it if you are going to try a ketogenic diet. Get yourself a quality blood ketone meter. Do not rely on urine sticks as they are inaccurate and primarily just detect the presence of ketones but have such varying ranges that it cannot be relied upon accurately. Utilizing your glucose monitoring device or your Dexcom and a blood ketone meter will aid you in determining your insulin needs if you are T1D. DKA typically starts when ketone levels encroach on or are >3mmol/L. Most people on ketogenic diets usually vary between .05-1.5mmol/L so there is little danger if adhering to proper keto principles and insulin management. This is why it is important to be guided by your Doctor or a health professional who knows what they are doing.
Why bother?
Chronically elevated blood sugar leads to greater requirements for insulin for both T1D & T2D’s. Chronic Hyperinsulinemia may eventually lead to obesity, higher triglyceride levels, and metabolic syndrome related diseases like heart disease and stroke. By focusing on controlling your insulin levels, not by consuming more of it, but by reducing the need for it, will vastly reduce your risk for advanced disease, and greatly enhance your quality of life.
Can a T1D also be a T2D?
A resounding YES. An uncontrolled management of T1D by eating a diet high in carbs/sugar will increase your needs for insulin dramatically. Chronically elevated levels of insulin will lead to conditions consistent with T2D. Eventually, an insulin dependent T1D will also suffer from the same conditions that plague an uncontrolled T2D. Take that to the bank!